Amy Stephens
MS, RDN, CSSD, CEDS
Licensed dietitian
specializing in sports nutrition
and eating disorders
MS, RDN, CSSD, CEDS
Licensed dietitian
specializing in sports nutrition
and eating disorders
Eating disorders affect an athlete both mentally and physically and have significant impacts on performance. This blog will discuss the prevalence of eating disorders, identify warning signs in athletes, distinguish the differences and similarities to relative energy deficiency syndrome (REDS), and provide resources for those struggling to seek help. Eating Disorders are a serious issue for everyone, but especially for athletes. Nutrition requirements are high and the inability to fuel an athlete’s body will lead to worsening of disordered eating, injuries, and overall decline in performance.

The most common forms of eating disorders are anorexia, bulimia and binge eating disorder. Anorexia refers to restriction of food and refusal to meet nutritional needs, typically resulting in extreme weight loss. Bulimia is defined by consuming a large quantity of food in a short period of time, followed by a desire to “get rid” of the food through vomiting, exercise, or medications. Often, athletes can have a combination of both. Binge eating disorder is another type of eating disorder characterized by consuming a large quantity of calories in a short period of time. In one study, up to 84% of athletes were found to have subclinical disordered eating, and engaging in maladaptive eating and weight control behaviors, such as binge eating, excessive exercise, strict dieting, fasting, self-induced vomiting, and the use of weight loss supplements (Chatterton, Clifford). Evaluation by a physician or therapist can determine the severity and best form of treatment.
Eating disorders do not discriminate as they affect all races, genders, and socioeconomic classes. Some populations have higher rates of eating disorders. Eating disorders are most commonly screened and diagnosed between the ages 12-19, but can occur at any age. The earlier an athlete is diagnosed, the more likely they are to recover and reverse any damage to their bodies. The longer an eating disorder behavior is untreated, the more difficult the treatment and full recovery become.
Prevalence
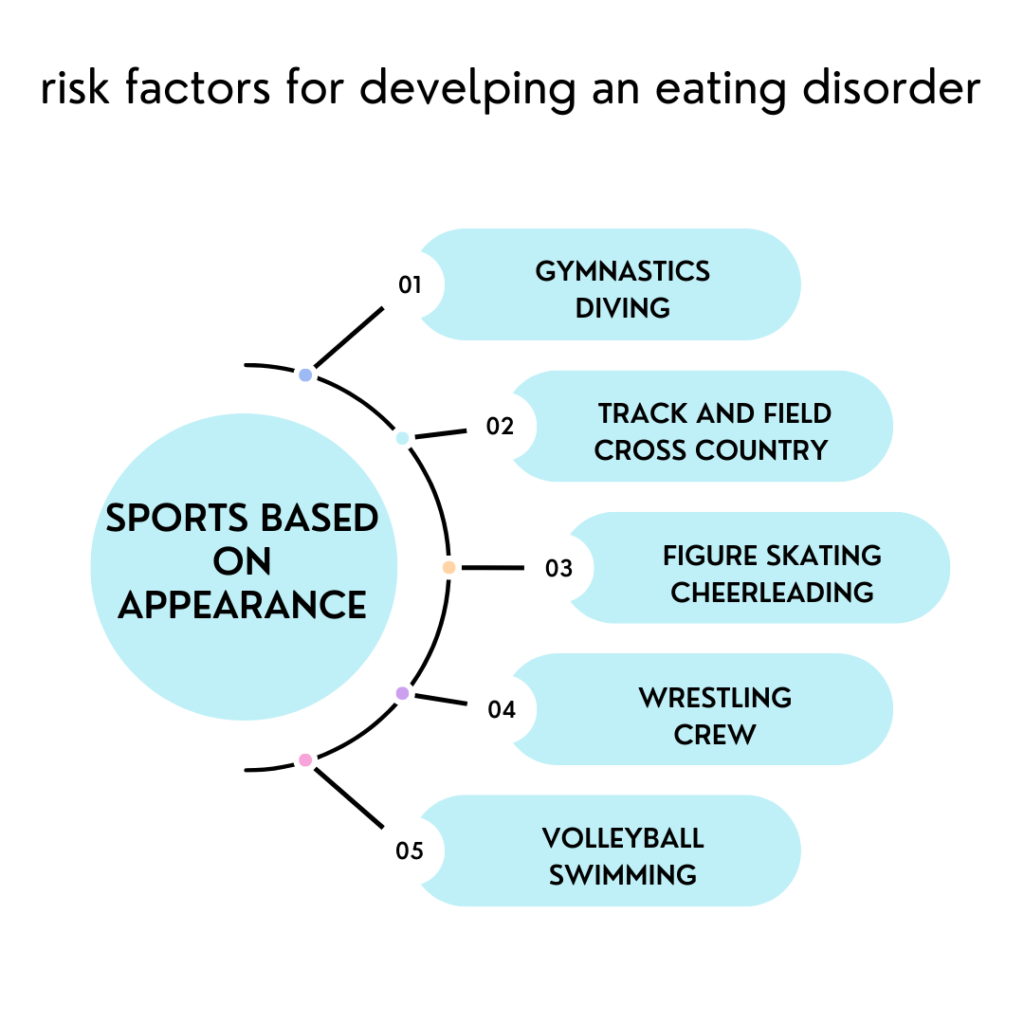
Risk factors for developing eating disorders in athletes
Certain sports that are weight dependent and focus on leanness pose a bigger risk for eating disorders. Both male and female athletes are at risk.
In addition, athletes who have recently undergone stressful events such as an injury are at a greater risk for developing an eating disorder. Athletes who have been struggling with poor performance might want to restrict food and blame the body.
There are additional societal contributions that can lead to eating disorders. It’s important to be aware of these factors so proper education for athletes and coaching staff can help prevent disordered eating among athletes.
Societal contributions include:
All of these practices promote unhealthy relationships with the body and eating patterns. Athletes are no exception. Weight dependent sports not only encourage unhealthy dietary practices, but reward them. The thinner athletes promote themselves as having reached their performance levels due to their thin body type. Misinformation from friends, coaches, and media can cause an athlete to try and achieve an inappropriate level of thinness that causes physical and mental harm to their body. Eating disorders are often overlooked if the athlete is performing well.
Difference between eating disorders and Relative Energy Deficiency Syndrome (RED-S)
Relative Energy Deficiency Syndrome (REDS) is a new classification of symptoms identified in 2014 by International Olympic Committee Mountjoy. REDS is characterized by low calorie intake in relation to energy exerted during exercise. REDS was formerly named “The Female Athlete Triad Syndrome because it affected three key systems in the female body:low calorie intake, menstrual irregularities, and lowered bone density. The term REDS is new but the condition has been in existence for a long time. Simply put, exercising too much and not eating enough causes an imbalance in which the body cannot function at optimal levels. What’s most interesting to me is that someone with REDS can be any body weight. The difference between REDS and an ED is that REDS is an unintentional mismatch of calories. Once an athlete with REDS is evaluated and educated about an appropriate amount of calories to sustain daily exercise and body functions, the deficit is corrected and the body can function properly. ED is further explored if the athlete is unable to willingly consume calories to support energy expenditure.
Sometimes it may not be obvious or easy to diagnose REDS or eating disorders. Someone can be a normal weight but is exercising too much and refueling inadequately. In this instance, athletes may feel that they are eating well, but in truth, are not eating enough calories to support exercise.
Females – change in menstrual cycle, can be longer or lighter periods, it is NOT normal for a female athlete to miss a period
Males – low testosterone and growth hormone. Both are natural performance enhancing hormones made by the body. Low levels can negatively affect sport performances, muscle growth, and energy production. Also important for serotonin uptake for the brain, it can lift mood. (Skolnick)
Hormonal changes can lead to stress fractures and ultimately osteoporosis
Frequent injuries to bones and soft tissues
Isolated, eats alone
Withdrawn behavior
Sudden changes with diet or food choices
Noticeable fluctuations in weight, both up and down
Irritability
Lethargy, difficulty finishing a workout
Digestive issues such as bloating (often mistaken for IBS), gas, diarrhea (this is often worsened by further restricting suspected nutrients)
Decrease in sports performance
Difficulty sleeping
Not seeing improvements in performance despite increasing workouts
Depressed immune system
Decreased cognitive functioning (lower blood sugar supplied to brain)
Treatment
Treatment often begins with an evaluation by a physician, eating disorder dietitian, and therapist. Once the patient is evaluated, they are recommended to the best form of treatment depending on their situation. The dietitian will create a plan that provides adequate calories to support daily expenditure. It can be challenging to find the right physician to help especially since there are differing opinions among professionals. In my experience, missing a period leads to complications related to menstrual cycle and bone growth. It is important to let your doctor know if you’ve lost your period for more than three months as this can be related to underfueling or the result of underlying medical conditions. Your doctor can help guide you to the best treatment approach.
Resources for help
There are many resources to help. If you or someone you are close to might have an eating disorder, here are some important resources that can help:

References
Bratland-Sanda S, Sundgot-Borgen J. (2013). Eating disorders in athletes: overview of prevalence, risk factors and recommendations for prevention and treatment. Eur J Sport Sci, 13(5):499-508.
Chatterton, J. M., & Petrie, T. A. (2013). Prevalence of disordered eating and pathogenic weight control behaviors among male collegiate athletes. Eating Disorders, 21(4), 328-341.
Clifford, T., & Blyth, C. (2018). A pilot study comparing the prevalence of orthorexia nervosa in regular students and those in university sports teams. Eating and Weight Disorders – Studies on Anorexia, Bulimia and Obesity, 24(3), 473-480.
Conviser, J. H., Schlitzer Tierney, A., Nickols, R. (2018). Essential for best practice: treatment approaches for athletes with eating disorders. J of Clin Sports Psych, 12.
Ghoch, M. E., et al. (2013). Eating disorders, physical fitness, and sport performance: a systematic review. Nutrients, 5:12.
Mehler, P.S., Sabel, A.L., Watson, T. and Andersen, A.E. (2018). High risk of osteoporosis in male patients with eating disorders. Int. J. Eat. Disord, 41: 666-672.
Mountjoy M, Sundgot-Borgen JK, Burke LM, et al. (2018). OC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Brit J of Sports Med, 52:687-697.
Petrie, Trent, Greenleaf, Christy, Reel, Justine, Carter, Jennifer. (2018). Prevalence of Eating Disorders and Disordered Eating Behaviors Among Male Collegiate Athletes. Psych of Men & Masculinity, 9: 267-277.
Scott CL, Plateau CR, Haycraft E. (2020). Teammate influences, psychological well-being, and athletes’ eating and exercise psychopathology: A moderated mediation analysis. Int J Eat Disord, 53(4):564-573.
Shufelt CL, Torbati T, Dutra E. (2017). Hypothalamic Amenorrhea and the Long-Term Health Consequences. Semin Reprod Med, 35(3):256-262.
Skolnick A, Schulman RC, Galindo RJ, Mechanick JI. (2016). The endocrinopathies of male anorexia nervosa: case series. AACE Clin Case Rep, 2(4):e351-e357.